
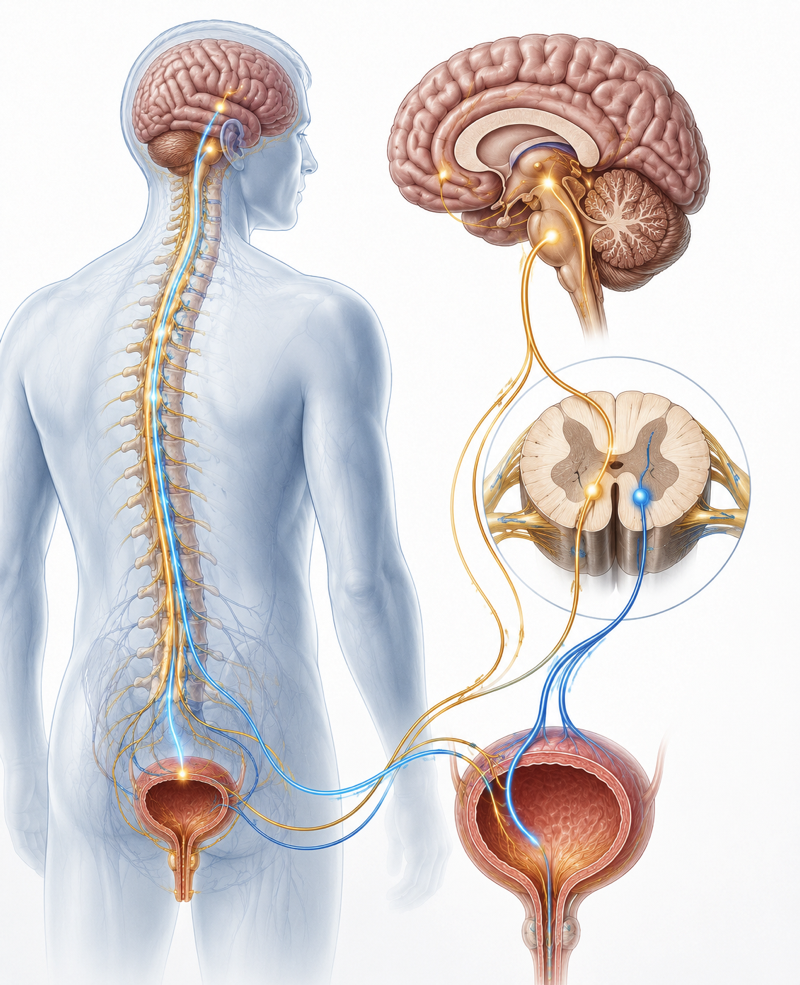
The bladder is, in essence, a sophisticated collaboration between muscle and nerves. The detrusor muscle stores urine and empties it on command — but that command comes entirely from a complex network of nerve signals coordinated between the brain, spinal cord, and peripheral nerves. When any part of that neural circuitry is damaged or disrupted, the result is neurogenic bladder — a condition where the bladder loses normal voluntary control and begins to behave erratically, dangerously, or both.
Neurogenic bladder is not a single diagnosis. It is an umbrella term covering a wide spectrum of bladder dysfunction caused by neurological disease or injury. Its management is one of the most complex areas in urology — requiring careful evaluation, tailored treatment, and ongoing surveillance to protect not just bladder function, but kidney health over the long term.
What Is Neurogenic Bladder?
A neurogenic bladder is any bladder dysfunction that results from impaired nerve control — whether from disease of the brain, spinal cord, or peripheral nerves supplying the bladder and sphincter. Depending on the level and nature of the neurological lesion, neurogenic bladder can manifest as:
- Overactive (hyperreflexic) bladder: Involuntary, uncontrolled bladder contractions leading to urgency, frequency, leakage, and in severe cases, dangerously high bladder pressures that threaten kidney function.
- Underactive (acontractile) bladder: The bladder muscle fails to contract adequately, leading to incomplete emptying, urinary retention, overflow incontinence, and recurrent UTIs from stagnant urine.
- Detrusor-sphincter dyssynergia (DSD): The bladder muscle and urethral sphincter contract simultaneously instead of in coordination — creating high pressure against a closed outlet. This is the most dangerous pattern because of the risk of progressive kidney damage from sustained high pressures.
Common Causes of Neurogenic Bladder
Neurogenic bladder can result from any condition that disrupts the neurological pathways controlling bladder function:
Spinal Cord Injury
The most common cause of neurogenic bladder in young adults. The pattern of bladder dysfunction depends on the level and completeness of the injury. Injuries above T6 cause overactive bladder with DSD risk. Lower thoracic and lumbar injuries typically cause an underactive bladder. All spinal cord injury patients require lifelong urological surveillance.
Multiple Sclerosis (MS)
Bladder symptoms affect 50-90% of MS patients during their disease course — often presenting before the diagnosis is established or changing as the disease progresses. Both overactive and underactive patterns can occur, sometimes alternating. MS-related bladder dysfunction is a major determinant of quality of life in affected patients.
Parkinson’s Disease
Overactive bladder is the most common urological manifestation of Parkinson’s disease — occurring in up to 70% of patients. The loss of dopaminergic inhibitory control leads to uninhibited detrusor contractions. Treatment is complicated by the overlap of bladder symptoms with the tremor and rigidity of the disease itself.
Diabetes Mellitus
Diabetic cystopathy — neurogenic bladder caused by diabetic autonomic neuropathy — is one of the most underrecognised complications of long-standing diabetes. It typically presents as an underactive, poorly contracting bladder with large residual urine volumes, overflow incontinence, and recurrent UTIs. Many patients are unaware they are not fully emptying their bladder.
Stroke
Overactive bladder with urgency incontinence is common after stroke — occurring in over 50% of patients in the acute phase. Many improve over time as neurological recovery progresses, but persistent neurogenic bladder after stroke is common and warrants specific urological management.
Spina Bifida and Congenital Spinal Anomalies
Children born with myelomeningocele (spina bifida) almost universally have neurogenic bladder — often with DSD and high bladder pressures that pose significant risk to kidney function from birth. Early urological evaluation and lifelong surveillance are essential.
Why Neurogenic Bladder Is a Threat to Kidney Health
This is the aspect of neurogenic bladder that is most critical to understand. An overactive bladder generating high pressures, or a bladder with DSD creating obstruction to outflow, can transmit those high pressures backwards to the kidneys through the ureters — causing hydronephrosis (kidney swelling), vesicoureteral reflux, recurrent kidney infections, and over time, irreversible kidney damage.
This is why neurogenic bladder is not just a quality of life issue — it is a kidney preservation issue. Regular monitoring of upper tract status (kidney function, imaging) is non-negotiable in any patient with a high-risk neurogenic bladder pattern.
Diagnosis and Assessment
- Urodynamic studies: The cornerstone of neurogenic bladder assessment. Cystometry measures bladder pressures during filling and voiding — identifying the pattern of dysfunction (overactive, underactive, or dyssynergic) and quantifying the risk to the upper tracts.
- Video urodynamics: Combines pressure measurement with fluoroscopic imaging of the bladder and urethra — the gold standard for neurogenic bladder assessment in high-risk patients.
- Post-void residual measurement: Ultrasound-guided assessment of residual urine volume after voiding.
- Renal ultrasound and function tests: Regular monitoring of kidney size, hydronephrosis, and GFR.
- Urine culture: Surveillance for UTI in patients with known incomplete emptying.
Treatment of Neurogenic Bladder
Clean Intermittent Catheterisation (CIC)
The cornerstone of management for underactive or retention-type neurogenic bladder. The patient (or carer) passes a clean catheter every 4-6 hours to empty the bladder completely — preventing overdistension, reducing infection risk, and protecting the upper tracts. CIC is safe, effective, and compatible with a full, active life when properly taught and practised.
Anticholinergic Medications and Mirabegron
Used to reduce overactive detrusor contractions — lowering bladder pressures, reducing urgency and leakage, and protecting the upper tracts in patients with high-pressure neurogenic overactivity.
Botulinum Toxin (Botox) Bladder Injections
Highly effective for neurogenic overactive bladder not adequately controlled by oral medications. Injections directly into the bladder wall reduce involuntary contractions, lower bladder pressures, and significantly improve continence and quality of life. Effects last 6-12 months, with repeat treatments as needed.
Sacral Neuromodulation
Electrical modulation of the sacral nerve roots — surgically implanted — can restore more normal bladder behaviour in selected patients with neurogenic bladder, particularly those with underactive patterns or refractory urgency incontinence.
Surgical Options
For patients with severely non-compliant, high-pressure neurogenic bladders unresponsive to other measures — augmentation cystoplasty (bladder enlargement using bowel) reduces bladder pressures and protects the kidneys. Urinary diversion may be required in selected severe cases. These are major surgical procedures considered only after all other options have been exhausted.
Lifelong Care Is the Foundation
Neurogenic bladder is a lifelong condition in most cases. Its management is not a one-time intervention but an ongoing programme of surveillance, treatment adjustment, and kidney protection — adapting as the underlying neurological condition and bladder behaviour change over time.
Dr. Prarthan Joshi at Zydus Hospitals, Ahmedabad, offers comprehensive neurogenic bladder evaluation — including video urodynamics, Botox bladder injections, and surgical management — for adults and children with all forms of neurological bladder dysfunction. For expert Neurogenic Bladder Treatment in Ahmedabad that protects both your bladder and your kidneys for the long term, consult Dr. Joshi today.