
Not every kidney stone can be managed with the gentlest approach. While small stones often pass on their own and medium-sized stones may be fragmented with shock wave therapy, large, complex, or strategically located stones require something more decisive — a minimally invasive surgical procedure that goes directly to where the stone is and removes it completely.
Two procedures represent the modern standard for surgical kidney stone management: Percutaneous Nephrolithotomy (PCNL) for large renal stones, and Ureteroscopy with Laser Lithotripsy (URS) for ureteric and selected kidney stones. Understanding what each involves, who they are right for, and what outcomes to expect removes much of the anxiety that comes with hearing the word “surgery” in the context of kidney stone treatment.
Why Some Stones Cannot Be Left to Pass or Shattered with ESWL
The management of kidney stones is not one-size-fits-all — it is guided by the size of the stone, its location within the urinary tract, its composition, the degree of obstruction it is causing, and whether infection is present. Stones that typically require surgical intervention include:
- Stones larger than 2cm in the kidney — too large to fragment effectively with ESWL and too large to pass even if fragmented.
- Staghorn calculi — large, branched stones that fill the kidney collecting system. These almost always require PCNL.
- Stones causing significant urinary obstruction — particularly when associated with hydronephrosis (kidney swelling) or infection, which represents a urological emergency.
- Stones that have failed ESWL — either not fragmenting or fragments not clearing.
- Ureteric stones causing persistent obstruction and pain not resolving with conservative management.
- Stones in kidneys with structural abnormalities where spontaneous passage is unlikely.
Percutaneous Nephrolithotomy (PCNL): Removing Stones Directly from the Kidney
PCNL is the gold standard surgical treatment for large kidney stones — stones over 2cm, staghorn calculi, and complex cases involving multiple stones or structural kidney abnormalities. The name describes the procedure: percutaneous (through the skin), nephro (kidney), lithotomy (stone removal).
How PCNL Works
Under general or spinal anaesthesia, a small puncture is made through the skin of the back directly into the kidney under real-time X-ray or ultrasound guidance. A working channel (tract) is dilated through this puncture to approximately 10mm, and a nephroscope — a specialised rigid endoscope — is introduced directly into the kidney collecting system. The stone is visualised directly, fragmented using pneumatic, ultrasonic, or laser energy, and the fragments systematically removed through the working channel. A temporary drainage tube (nephrostomy) is placed at the end of the procedure.
Mini-PCNL and Ultra-Mini PCNL
Advances in instrument design have produced miniaturised versions of PCNL using smaller working channels (4.8-5mm for mini-PCNL, even smaller for ultra-mini). These reduce the invasiveness of the procedure, decrease blood loss, and allow day-case or shorter hospital stay for selected patients — while maintaining effective stone clearance for stones that would previously have required standard PCNL. The choice between standard and miniaturised PCNL depends on stone size, complexity, and kidney anatomy.
Results and Recovery
Stone-free rates for PCNL in large renal stones exceed 85-90% in experienced hands — significantly higher than ESWL for stones of the same size. Hospital stay is typically 2-3 days. The nephrostomy tube is usually removed within 24-48 hours once drainage is clear. Most patients return to normal activities within 2-3 weeks. Compared to open stone surgery of decades past, PCNL is transformatively less invasive — with substantially lower blood loss, shorter hospital stay, and far faster recovery.
Ureteroscopy with Laser Lithotripsy (URS-LL): The Keyhole Approach
Ureteroscopy with Holmium laser lithotripsy is the treatment of choice for most ureteric stones — whether in the upper, mid, or lower ureter — and for selected kidney stones, particularly those in the 1-2cm range where PCNL might be considered excessive and ESWL has failed or is unlikely to succeed.
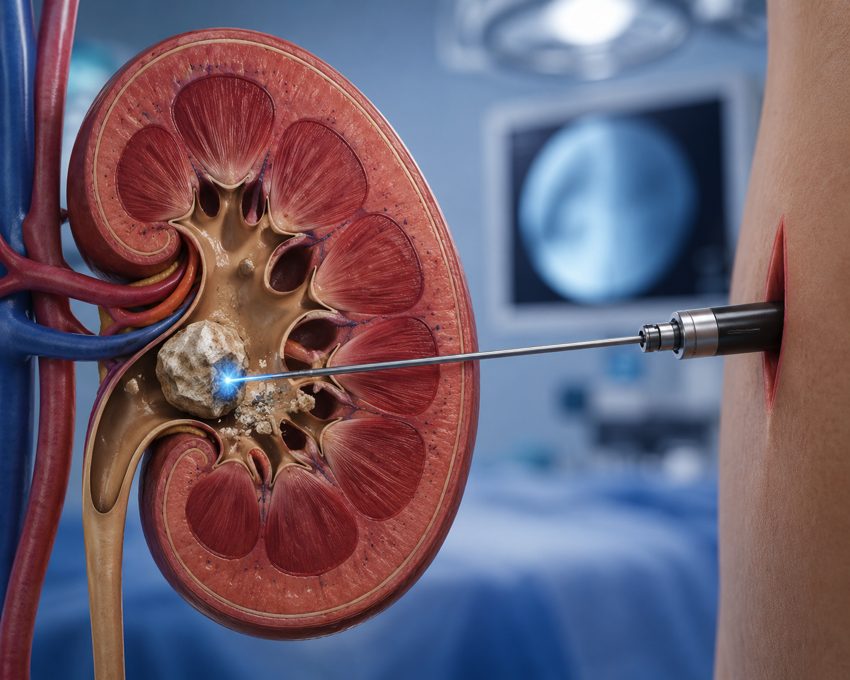
How URS-LL Works
A thin, semi-rigid or flexible ureteroscope is passed through the urethra, into the bladder, and up the ureter to the stone under direct vision — no skin incision at all. A Holmium laser fibre is passed through the working channel of the ureteroscope and the laser energy precisely fragments the stone into either small passable pieces or fine dust (dusting technique), which clears spontaneously or is retrieved with a small basket. A temporary ureteric stent is usually placed at the end of the procedure to protect the ureter while healing occurs — this is removed in the clinic 1-2 weeks later.
Flexible Ureteroscopy (RIRS) for Kidney Stones
When the stone is located within the kidney rather than the ureter, a highly flexible digital ureteroscope can be advanced all the way into the kidney collecting system — accessing stones in areas that rigid instruments cannot reach. This technique, called Retrograde Intrarenal Surgery (RIRS), can effectively treat kidney stones up to 2cm (and sometimes larger with multiple sessions) with no skin incisions whatsoever. It is particularly valuable for patients with bleeding disorders, those on anticoagulants, and those in whom a skin puncture carries higher risk.
Choosing Between PCNL and URS: How the Decision Is Made
The choice between PCNL and ureteroscopic laser treatment is guided by stone size, stone location, kidney anatomy, and patient health:
- Stones over 2cm in the kidney: PCNL (standard or mini) is first choice.
- Staghorn or branching stones: Standard PCNL, sometimes staged (multiple sessions).
- Ureteric stones of any size: URS with Holmium laser is first choice — no skin puncture needed.
- Kidney stones 1-2cm: Either RIRS (flexible ureteroscopy) or mini-PCNL depending on stone density, location, and patient factors.
- Kidney stones under 1cm: ESWL or RIRS depending on stone density and location.
For complex cases — multiple stones, horseshoe kidneys, prior pelvic or kidney surgery — a staged approach combining techniques may be planned. A skilled urologist discusses all options transparently and recommends the most appropriate pathway for each patient’s specific stone burden.
Stone Prevention After Surgery
Surgery removes the stone — but it does not prevent the next one. Metabolic evaluation after a significant stone event guides long-term prevention: 24-hour urine collection, blood tests for calcium and uric acid, stone composition analysis. Targeted dietary changes, hydration goals, and where needed specific medications (potassium citrate, thiazide diuretics, allopurinol) dramatically reduce recurrence rates.
Dr. Prarthan Joshi at Zydus Hospitals, Ahmedabad, offers the complete range of modern kidney stone surgical treatments — from mini-PCNL and standard PCNL to flexible ureteroscopy and Holmium laser lithotripsy — with a dedicated focus on stone-free outcomes and long-term prevention. For expert Kidney Stone Surgery in Ahmedabad, consult Dr. Joshi today.