
When a patient is told that blood in their urine has led to the suspicion of bladder cancer, the conversation that follows is often frightening and confusing. Staging investigations, grading, cystoscopy, TURBT — a cascade of unfamiliar terms arrives at a moment of significant anxiety. Yet understanding the procedure at the centre of early bladder cancer management — Transurethral Resection of Bladder Tumour, or TURBT — reveals something genuinely reassuring: for non-muscle invasive bladder cancer, this single procedure both confirms the diagnosis and, in many cases, delivers the initial treatment.
TURBT is one of the most important procedures in uro-oncology. It is performed through the urethra — no external incisions — and is the cornerstone of bladder cancer management for the large majority of patients whose cancer has not yet invaded the muscular wall of the bladder. Understanding what it involves, what it achieves, and what follow-up it requires gives patients the clarity and confidence they need at a difficult time.
Why TURBT Is Both Diagnostic and Therapeutic
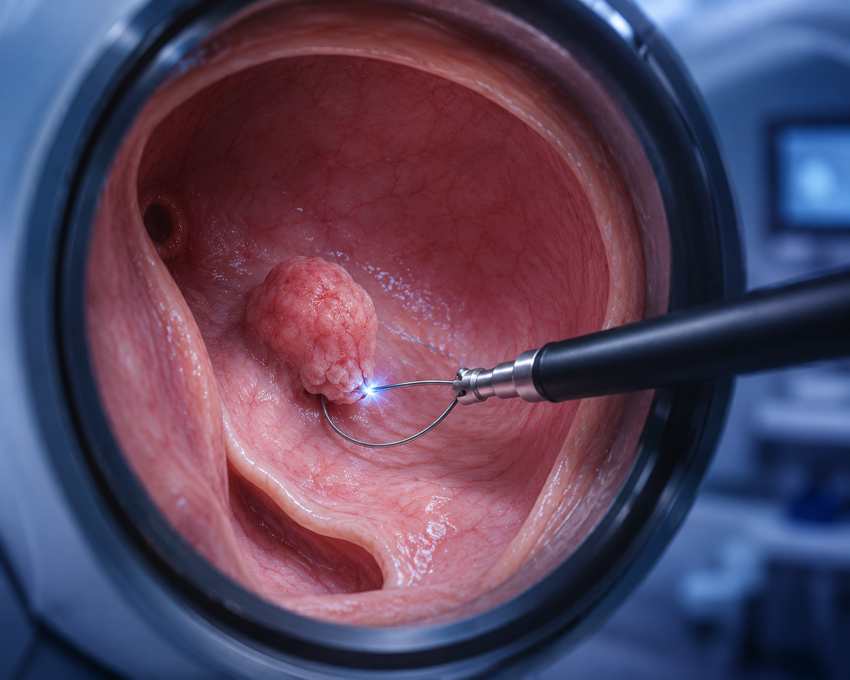
Unlike most cancer biopsies where the aim is simply to obtain tissue for analysis, TURBT is designed to remove the visible tumour completely — not just sample it. The resectoscope passed through the urethra carries an electrosurgical loop that systematically resects the tumour and a portion of the underlying bladder muscle in layers — removing the lesion in its entirety while simultaneously sending tissue for pathological analysis.
The pathology report from TURBT provides three critical pieces of information that determine everything about subsequent management:
- Histological type: Confirming the tumour is urothelial carcinoma (or a rarer variant) and its grade — low-grade (less aggressive) or high-grade (more aggressive).
- Depth of invasion (T staging): Whether the tumour is confined to the inner lining only (Ta), has invaded the lamina propria (T1), or has reached the muscularis propria — the muscle layer (T2). This distinction between non-muscle invasive (Ta, T1) and muscle-invasive (T2+) disease is the most critical decision point in bladder cancer management.
- Presence of CIS (Carcinoma in Situ): A flat, high-grade lesion that is not raised or visible as a papillary tumour but carries high malignant potential — its presence changes subsequent treatment intensity significantly.
The TURBT Procedure: Step by Step
Preparation
TURBT is performed under spinal or general anaesthesia as an inpatient or day-case procedure. Pre-operative urine culture must confirm the absence of active infection. Blood tests including clotting profile are checked. Patients on anticoagulants require appropriate bridging as directed by their anaesthetist and urologist.
The Procedure
The patient is positioned with legs supported (lithotomy position). A resectoscope is introduced through the urethra into the bladder — the bladder is filled with irrigating fluid to provide a clear operating field. The urologist systematically resects the tumour using the electrosurgical loop, working from the superficial surface through the deeper layers, including a sample of the underlying detrusor muscle at the base to allow accurate T-staging. The resected chips are evacuated from the bladder and sent for histopathology. Bleeding vessels are coagulated under direct vision. The procedure typically takes 30-90 minutes depending on tumour size and number.
Post-Operatively
A urinary catheter is placed at the end of the procedure for bladder irrigation — running saline through the bladder to prevent clot formation. This is typically maintained for 12-24 hours. A single instillation of intravesical chemotherapy (mitomycin C) given within 24 hours of TURBT — before the catheter is removed — significantly reduces the risk of tumour reimplantation and early recurrence in non-muscle invasive disease. Most patients are discharged within 1-2 days.
Re-TURBT: When a Second Look Is Essential
International guidelines recommend a second TURBT (re-TURBT) 4-6 weeks after the initial procedure in two specific situations:
- High-grade T1 tumours: The risk of understaging — the tumour actually being deeper than T1 — is significant, and re-TURBT detects residual or invasive disease in up to 30-40% of cases.
- Incomplete initial resection: When the initial TURBT was technically incomplete due to tumour size, location, or bleeding.
Re-TURBT is not a sign that the first procedure failed — it is a deliberate, guideline-recommended quality measure that ensures the most accurate staging and the most complete initial treatment.
After TURBT: Intravesical Therapy and Surveillance
TURBT treats the visible tumour — but bladder cancer has a high recurrence rate. The field change theory suggests that the entire bladder urothelium may be at risk. Post-TURBT management depends on the risk stratification of the tumour:
Low-Risk Non-Muscle Invasive Bladder Cancer
Single, small, low-grade Ta tumour. After TURBT with single immediate mitomycin C instillation, surveillance cystoscopy at 3 months, then annually for 5 years. Most patients with low-risk disease do not recur at high grade or progress to muscle-invasive disease.
Intermediate-Risk Non-Muscle Invasive Bladder Cancer
Multiple or recurrent low-grade tumours. Adjuvant intravesical chemotherapy (mitomycin C) instillations for 6-12 months after TURBT. Regular surveillance cystoscopy at 3 months, 9 months, then annually.
High-Risk Non-Muscle Invasive Bladder Cancer
High-grade T1, carcinoma in situ, or large/multiple high-grade Ta tumours. Intravesical BCG (Bacillus Calmette-Guerin) immunotherapy — induction course of 6 weekly instillations followed by maintenance courses over 1-3 years. BCG significantly reduces recurrence and progression rates in high-risk NMIBC. Closer surveillance cystoscopy schedule. Persistent or progressive high-risk disease may require radical cystectomy (bladder removal) — a decision that requires detailed specialist discussion.
The Importance of Surveillance Cystoscopy
Bladder cancer surveillance cystoscopy is non-negotiable. The high recurrence rate of bladder cancer — even after complete initial TURBT — means that regular endoscopic inspection of the bladder is the only reliable way to detect recurrence early, when it is most easily and effectively treated. Missing surveillance appointments risks allowing a recurrence to progress to muscle-invasive disease — transforming a manageable condition into one requiring radical surgery.
Dr. Prarthan Joshi at Zydus Hospitals, Ahmedabad, offers comprehensive bladder cancer management — from urgent flexible cystoscopy and CT urogram for haematuria investigation, to TURBT, intravesical therapy administration, and long-term surveillance. For expert Bladder Cancer Treatment in Ahmedabad that combines clinical precision with genuine patient support throughout the entire treatment journey, consult Dr. Joshi today.